CTCAE COVERAGE850 criteria across v5.0 and v6.0
REGIMEN PROFILES42 oncology regimens (cytotoxic, targeted, immunotherapy, bispecific, CAR-T, ADC, radioligand)
ATTRIBUTIONWHO-UMC and Kramer, per-drug probability, reasoning path visible
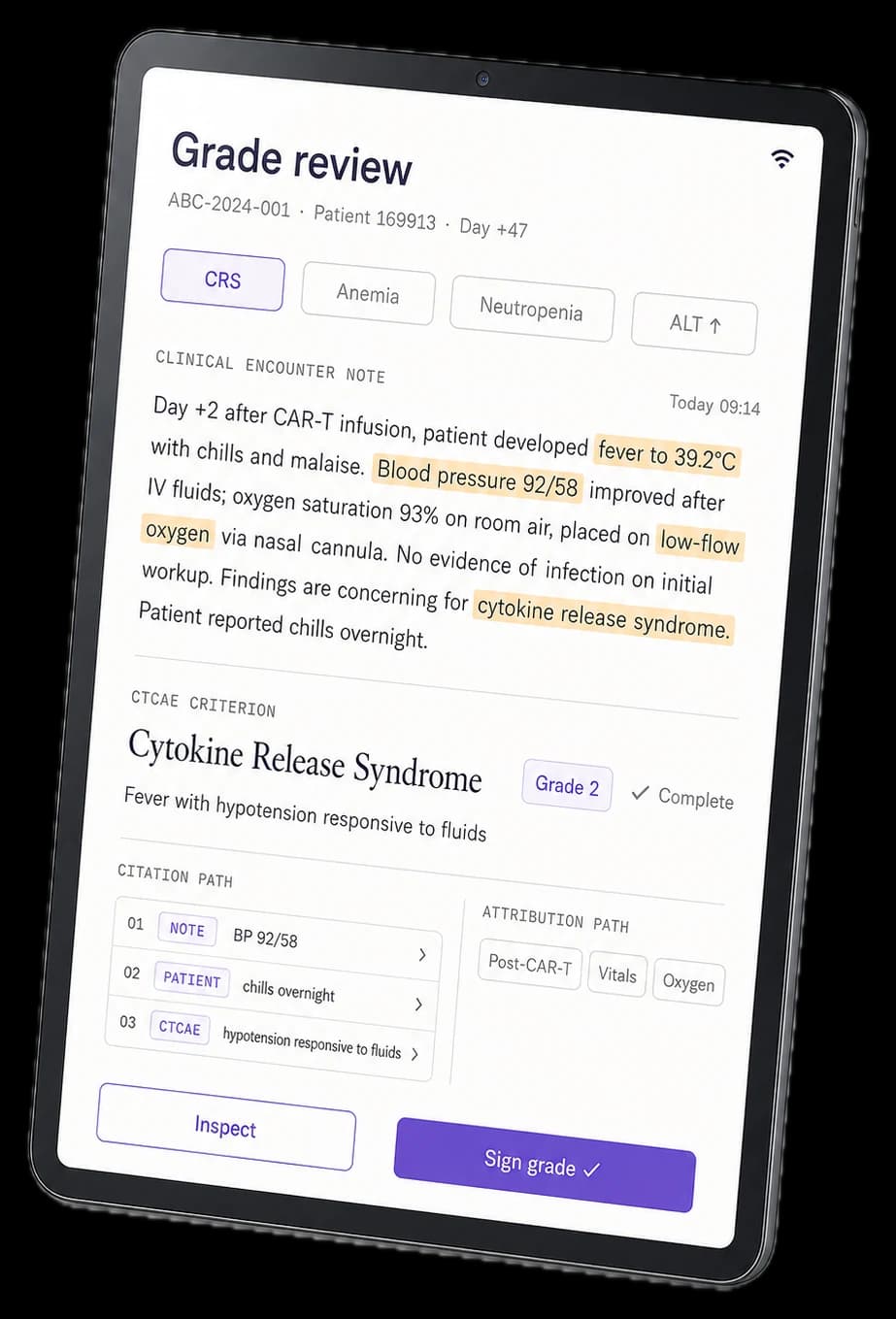
CITATIONSource sentence + CTCAE criterion required for every grade. Architectural constraint.
E-SIGNATURE21 CFR Part 11 trail captured automatically
LANGUAGESEnglish, French, German, Spanish, Portuguese, Italian, Japanese, Korean, Arabic
EHR INTEGRATIONSMART on FHIR R4 (Epic, Oracle Health, Athena, Allscripts, MEDITECH, Dedalus, Orbis, regional APAC)
EDC WRITEBACKMedidata Rave, Veeva Vault EDC, Oracle Clinical One
TIME PER EVENT17 minutes → under 3 minutes
COMPLIANCE21 CFR Part 11, GVP Module VI, HIPAA, GDPR. SOC 2 Type II in flight.