For Cancer Trial Research Directors
A safety operation your coordinators can stay in.
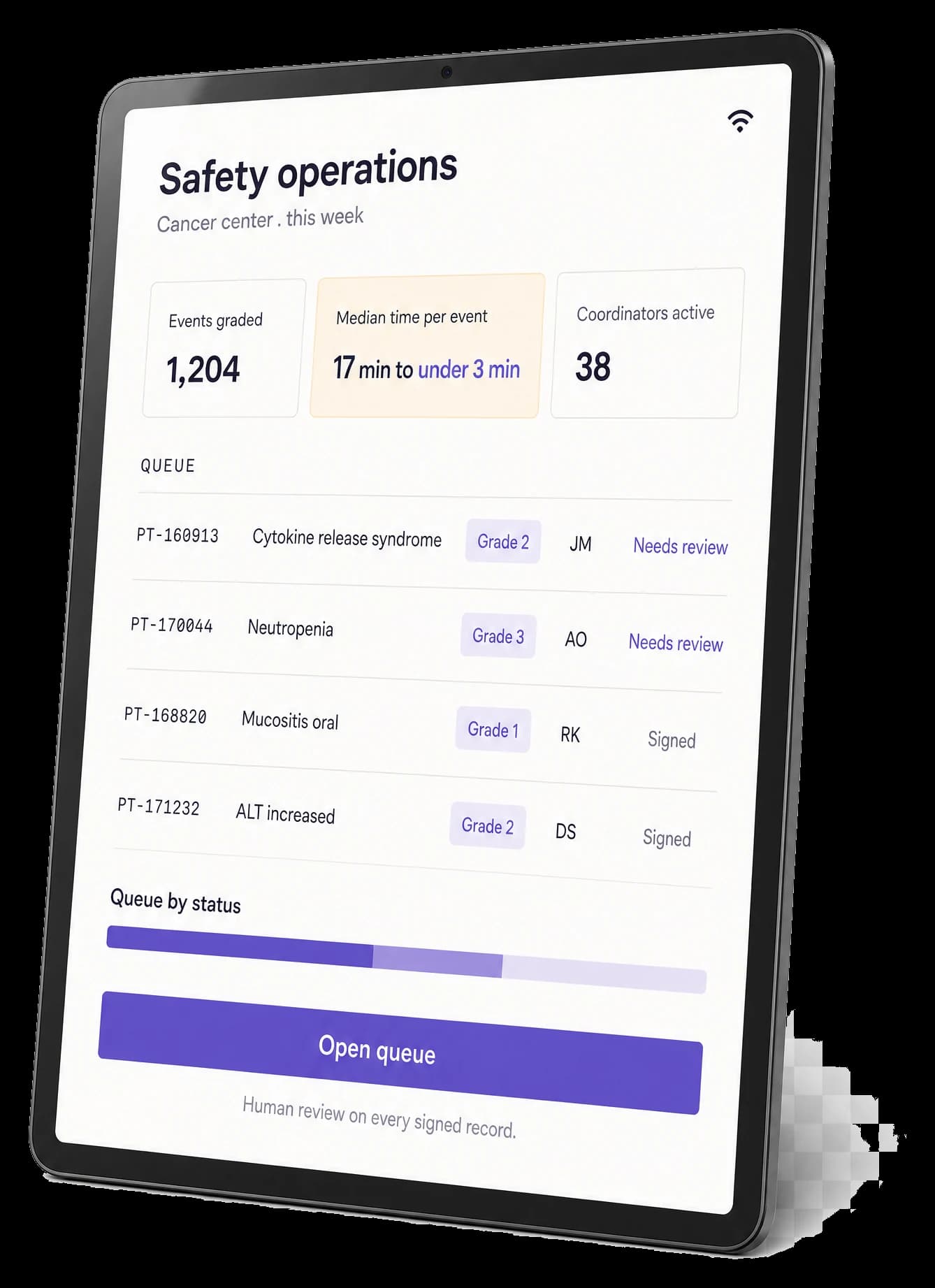
Burna handles the lookup so coordinators handle the judgment. Seventeen minutes per adverse event compresses to under three. New coordinators grade consistently from week one. The nine-year senior coordinator stays because the work is finally what she trained for.
SMART on FHIR inside Epic, Oracle Health (Cerner), and regional EHRs. 21 CFR Part 11 aligned. HIPAA, GDPR, and regional sovereignty options. CancerX member. FDA EDSTP application in review. Built for the unit that carries the audit findings and the next trial on the same calendar.
SMART on FHIR
Epic
Oracle Health
CTCAE v5 and v6
WHO-UMC
Kramer
21 CFR Part 11
SOC 2 Type II
HIPAA, GDPR
Medidata Rave
Veeva Vault
CancerX
SMART on FHIR
Epic
Oracle Health
CTCAE v5 and v6
WHO-UMC
Kramer
21 CFR Part 11
SOC 2 Type II
HIPAA, GDPR
Medidata Rave
Veeva Vault
CancerX
17→3 min
Per adverse event, with the source sentence, CTCAE criterion, and attribution path attached.
$192K–710K
Per-trial query labor at industry-standard rates (Oracle ClearTrial, 2021). Approximately 85% structurally closeable.
90-day pilot
In success, the labor recovery the platform was scoped to produce. If endpoints are not met, the contract terminates with no further fee; the unit retains the work product.
The validation endpoints I co-designed for Burna are the endpoints I would have wanted to see as a sponsor’s CMO before pilot kickoff. Pre-registered, peer-reviewed, paired-grader timing. The science is the procurement asset.
Dr. Andrea PirzkallFormerly Chief Medical Officer at Replimune and Asher Biotherapeutics; Executive Director Clinical Development at BeiGene; Principal Medical Director at Genentech
EHR · NOTECTCAE v5.0 PDFLABSAE FORM
- 01Reads progress note in EHR
- 02Opens CTCAE v5.0 PDF in new tab
- 03Scrolls through 850 criteria for "neutropenia"
- 04Reads 4 grade definition thresholds
- 05Switches to labs tab to find ANC
- 06Finds ANC 780 → Grade 3
- 07Writes attribution + severity + outcome
- 08Drafts narrative · closes encounter
NeutropeniaGrade 3
ANC 780 on 2026-04-12 08:17 · CTCAE v5.0 criterion
WHO-UMC Probable → FOLFIRINOX
- 01Opens encounter in Epic
- 02Burna surfaces the AE inline
- 03Click "show me why" → citation expands
- 04Sign · flows to Medidata · narrative drafted
Sign · forward to Medidata
→−15 minutes per adverse event · 88% coordinator time recovered
The Pilot
The shape of a Burna pilot.
Every Burna pilot follows the same four-phase structure, designed for academic medical center procurement and IRB timelines. The pilot is a co-designed scientific engagement. The output is a peer-reviewed manuscript with your unit as primary authors. The deliverable is a workflow study with pre-registered endpoints.
Every cancer center clinical research director reading this page already knows the math. The unit runs 80 to 200 active oncology trials. The senior coordinator has been there nine years and is starting to receive calls from industry. Three coordinators are still learning CTCAE and producing the kind of grading inconsistencies that turn into corrective action plans. The next trial is already on the calendar. The 90-day pilot is built for the unit she actually runs, not the unit a vendor wishes she ran.
PHASE 1
Weeks 1–3
Scoping
Your CIO, your CISO, your Director of Clinical Trials, and your IRB lead meet with Burna’s engineering and clinical team. The workflow study is co-designed: paired-grader timing, documentation completeness, and attribution agreement endpoints. Data residency and SMART on FHIR integration scope are finalized. Training rollout and change management are agreed. The Master Service Agreement, Business Associate Agreement, and study protocol are executed.
PHASE 2
Weeks 4–6
Integration
Burna registers as a SMART on FHIR app inside Epic, Oracle Health, or your regional EHR. Your IT provisions one OAuth client and one FHIR endpoint. Burna’s engineering team handles FHIR mapping, residency configuration, and EDC integration with Medidata Rave, Veeva Vault EDC, or Oracle Clinical One. The Implementation Lead arrives on-site for training and workflow walkthroughs. Test environments validate against your unit’s data.
PHASE 3
Weeks 7–18
In-Pilot
The unit runs Burna in production against the workflow study endpoints. Coordinators grade with Burna assistance; expert graders work the same cases blind. The Implementation Lead remains on-site or rotating-on-site through the pilot window. Weekly check-ins surface friction and resolve it. Monthly steering committee review with your Director, your CIO, and Burna’s clinical team.
PHASE 4
Weeks 19–21
Readout
Database lock. Statistical analysis. Manuscript co-drafting with your unit as primary authors and Burna as secondary. Decision point: enterprise contract, extended pilot, or you keep everything (the deployment, the training materials, the playbook, the manuscript) and walk away.
Pilot Outcome Terms
The terms the pilot ships under.
In success, the pilot delivers a citation-bound CTCAE workflow inside Epic, Oracle Health, or your regional EHR; the labor recovery the platform was scoped to produce; and a peer-reviewed manuscript with your unit as primary authors. The endpoints are pre-registered and co-authored with your CMO and Director before kickoff.
If the pre-registered workflow study endpoints are not met at study end, the contract terminates with no further fee, and your institution retains the deployment, the training materials, the change-management playbook, the Implementation Lead’s work product, and the co-authored manuscript. The team publishes together, or publishes the negative result. Either way, your unit is the named institution on a peer-reviewed paper.
This is possible because failed studies are still useful science. Most healthcare AI vendors cannot offer it because their commercial model depends on every pilot converting. Burna’s commercial model depends on the studies that succeed converting; the studies that do not still ship knowledge to the field.
The Playbook
What ships with every pilot.
Most oncology AI deployments ask the customer to figure out integration, training, change management, and workflow redesign on their own. Burna ships the work. The 12-pillar Implementation Playbook is operationalized from real oncology deployments and built into every pilot.
Clinical Safety
Regulatory Alignment
Change Management
Training and Learning
Communications
Workflow Embedding
Policy and Governance
Support and Troubleshooting
Monitoring and Optimization
Data Reporting
Continuity and Scaling
LMS-compatible training modules in your authoring system. Communication templates for your medical executive committee, your IRB, your sponsor monitors, your DSMB. Future-state workflow maps for coordinators, MDs, PIs, and CRAs.
Governance and policy guidance for your Office of Research and your CISO. An on-the-ground Implementation Lead for the full pilot window. Your team arrives ready, with Burna alongside.
For your CIO, CISO, and General Counsel
Architecture, sovereignty, and procurement.
Three documents your security and procurement teams need on day one of scoping. Pre-negotiated, single-document downloads.
Download the 5-page brief →Architecture
SMART on FHIRSMART on FHIR app inside Epic, Oracle Health (Cerner), Athena, Allscripts, eClinicalWorks, MEDITECH, Dedalus Orbis, and regional systems. On-premises deployment inside your hospital network. Sponsor-tenant architecture for pharma and CRO engagements. Twelve-agent cascading constraint pipeline. Every grade requires a source sentence and a CTCAE criterion: architectural constraint, not runtime filter. Two patents filed.
Sovereignty
10+ regionsPatient identifiers stay inside your network in on-premises deployments, and inside your jurisdiction in regional cloud deployments. Regional residency at launch: US, EU (Frankfurt, Dublin, Paris), UK, Canada, Australia, Japan, Korea, Singapore, UAE, KSA. Sovereign cloud partnerships in negotiation for Oracle Australia, G42 UAE, and STC Saudi Arabia. The grading model only sees de-identified clinical text.
Procurement
Pre-negotiatedMSA, BAA, DPA, subprocessor list, insurance certificates, right-to-audit clause, source code escrow option, and 90-day exit and data export provisions are pre-negotiated, single-document downloads from the procurement portal. Your General Counsel reads them in a week, not a quarter. Standard FedRAMP Moderate-equivalent control set. SOC 2 Type II audit kicked off Q2 2026; Type I attestation available now.
Pricing
What this costs after the pilot.
Pilots are zero cost during the 2026 design partner cohort. Post-pilot enterprise pricing scales with seat count, trial volume, and postmarket surveillance scope.
Mid-size academic medical centers
$200K–$500K
Annually. Recommended for centers with 30 to 80 active oncology trials and 4 to 12 research coordinators. The anchor tier for the 2026 design partner cohort.
Major comprehensive cancer centers
$500K–$1.5M
Annually. Recommended for centers with 100+ active oncology trials, multiple sites, and dedicated oncology pharmacovigilance teams.
Regional pricing available
For centers in emerging markets where US pricing is unworkable. Multi-year contracts include built-in price protection through 2028.
Most cancer centers recoup year-one cost through coordinator capacity expansion alone. Per oncology trial query labor sits at $192K to $710K at industry-standard rates (Oracle ClearTrial, 2021), with approximately 85% structurally closeable per Pronker et al., 2011. Across a unit running 80 to 200 trials, that math compounds. The platform is the conversation, not the tool.
Validation
What evidence to expect.
Burna does not publish accuracy percentages on this page. They will be published in peer-reviewed venues. Target journals: JCO, JAMIA, JCO Clinical Cancer Informatics, Annals of Oncology. Until publication, methodology is available under NDA to pilot scoping conversations.
See /validation for full detail →STUDY 01
In flight, US cancer center
Prospective workflow study
Co-designed with Dr. Andrea Pirzkall (formerly CMO at Replimune and Asher Biotherapeutics, Executive Director Clinical Development at BeiGene, Principal Medical Director at Genentech).
STUDY 02
Retrospective, NCI-designated comprehensive cancer center
1,200-chart accuracy study
Bio-IT World 2026 poster. Pre-registered endpoints. Conservative reporting.
STUDY 03
Paired-grader structure
Second-site prospective pilot
Inside an active GI oncology and Phase 1 trials program.
STUDY 04
Launching 2027
Postmarket pharmacovigilance pilot
Postmarket signal detection and ICSR triage workflow study, target launch 2027.
Validation Principles
Pre-registered endpoints. Peer-reviewed target venues. Independent IRB or HREC oversight. Conservative reporting. External co-authorship. Pre-print on medRxiv within 60 days of database lock. Failed studies still publish.

“The validation study endpoints I co-designed for Burna are the endpoints I would have wanted to see as a sponsor’s CMO before pilot kickoff. Pre-registered, peer-reviewed target venues, paired-grader timing, multi-drug attribution agreement. The science is the procurement asset.”
Dr. Andrea PirzkallFormerly Chief Medical Officer at Replimune and Asher Biotherapeutics; Executive Director Clinical Development at BeiGene; Principal Medical Director at Genentech
The Bench
Who reviews the work.
Burna is advised by 25 oncologists, pharmaceutical executives, regulatory scientists, informaticists, and operators across 5 councils. The councils relevant to a cancer center evaluation:
Clinical Council
Dr. Andrea Pirzkall
Dr. Michel Azoulay (Strategic Advisor to the CEO; Exec Lead for Protocol Safe), Dr. Tehseen Salimi (Global CMO at Fresenius Medical Care; formerly SVP Medical Affairs at Taiho Oncology).
Commercial Council
Scott Schliebner
COO at P1 Pratia Oncology. Dr. John Hayslip (CMO at Verastem Oncology, formerly Director of Clinical Research at Markey Cancer Center).
Clinical Council
Dr. Stefan Gluck
Formerly VP at Celgene. Presenting Burna at AI in Oncology Germany, ESMO Breast Cancer, and ASCO 2026.
Regulatory & Standards Council
Dr. Howard Fingert
Formerly VP Medical Oncology at ONO Pharma USA; Senior Medical Director at Takeda. Trained at Dana-Farber and MGH.
Tech & Product Council
Dr. Joel Saltz and Dr. Mary Morison Saltz
SUNY Distinguished Professor and founding chair of Biomedical Informatics at Stony Brook. Chief Clinical Integration Officer at Stony Brook Medicine, led the N3C national data initiative.
Full advisor board
25+ advisors across 5 councils
Clinical operations, clinical trials, pharma, CRO and site networks, regulatory, informatics, governance, product, implementation, and commercial leads. Full board at /about.
Note: advisors are listed in their personal capacity. Affiliations are disclosed for context, not to imply institutional endorsement. Full advisory board at /about.
A Scene
What Monday looks like in your unit.
Monday morning in a cancer trial unit running Burna for three months. The senior coordinator opens her queue. Six adverse events landed over the weekend across four trials. Each one arrives with the source sentence highlighted, a suggested CTCAE grade, and the WHO-UMC or Kramer attribution path already worked out. She agrees on five and signs them in under fifteen minutes. She modifies one (the nausea is Grade 2, not Grade 1); her reasoning is logged with the edit, and the calibration improves quietly behind her work.
The three coordinators who joined six months ago are grading their first cycles independently. Their inconsistency rate is down meaningfully from week one. The senior coordinator reviews their work in five minutes per chart, not twenty. She is not the bottleneck the unit had quietly built itself around.
The Director’s Monday dashboard shows cross-site grading consistency up since pilot start, query closure cycle compressed, and three corrective action plans from the prior eighteen months now closed. The sponsor monitor for the lead trial has not opened a query in two weeks. The DSMB packet for the Phase 1 trial is one click from final.
The next sponsor RFP arrives Thursday.

“She is not the bottleneck the unit had quietly built itself around.”
FAQ
Cancer center questions.
The seven we hear most often from research directors. The full FAQ has the rest.
Read the full FAQ →How is this different from the prior generation of clinical AI?
The previous generation of clinical AI in oncology was broad, opaque, and made autonomous decisions. Burna is the opposite on every axis: narrow (CTCAE grading and multi-drug attribution only), transparent (every grade cites the criterion and the source text), and human-in-the-loop by design. Burna suggests; your clinicians decide.
How much can we expect to reduce queries by?
The 90-day pilot’s pre-registered endpoints typically include a target of 50% reduction in confirmation queries on adverse event forms. At industry-standard query rates of $192K to $710K per trial in query labor, with 85.7% of those queries being confirmation requests (Pronker et al., 2011), the structurally closeable labor per trial is meaningful at unit scale. The exact figure depends on your current baseline, which is one of the things the scoping conversation surfaces.
How long does integration actually take?
Two to three weeks from kickoff to first signed grade in your production environment. Your IT provisions one OAuth client and one FHIR endpoint. Burna’s engineering team handles the rest, including EDC integration with Medidata Rave, Veeva Vault EDC, or Oracle Clinical One.
Where does our patient data go?
Patient identifiers stay inside your network in on-premises deployments and inside your jurisdiction in regional cloud deployments. The grading model only sees de-identified clinical text. Architecture diagram in the 5-page brief.
Is this a medical device?
No. Burna is a clinical decision support tool. Clinicians approve every output. The platform does not prescribe, modify dose, or alter care pathways. 21 CFR Part 11, SOC 2, HIPAA, and GDPR aligned.
Do you support our EHR?
SMART on FHIR runs inside Epic, Oracle Health (Cerner), Athena, Allscripts, eClinicalWorks, MEDITECH, Dedalus (France, Italy, Spain), AGFA Orbis (Germany, Benelux), and regional APAC systems. If your EHR supports FHIR R4, Burna runs inside it.
What about our sponsor monitors and our CROs?
Burna produces a monitor-readable audit trail by default. Your CRO sees the same evidence chain your coordinator saw: source sentence, CTCAE criterion, attribution trail, correction history, and e-signature. Faster query closure.
Final
Bring Burna into your next trial cohort.
Pilot scope, endpoints, publication path, training materials, and governance artifacts are defined before kickoff. The Master Service Agreement and Business Associate Agreement are pre-negotiated single-document downloads. The workflow study is co-designed around the operational measurements your unit already tracks.
2026 Design Partner Cohort
Pilot scoping for cancer trial units, through Q3 2026
The 2026 design partner cohort accepts pilot scoping conversations through the end of Q3 2026. Pilots that begin in Q4 2026 ship co-authored manuscripts in late 2027.
In success, your unit gets a citation-bound CTCAE workflow inside the EHR, the labor recovery the platform was scoped to produce, and a peer-reviewed manuscript with your unit as primary authors. If the pre-registered endpoints are not met at study end, the contract terminates with no further fee, and your unit retains the deployment, the playbook, and the manuscript. Either way, your team publishes.
Architecture and Implementation
Download the 5-page brief
Five pages your CIO, CISO, and General Counsel can read in one sitting. Architecture diagram, sovereignty configuration, BAA, DPA, and 90-day exit and data export provisions.
Mutual NDA available on request.
For pilot scoping conversations later in 2026.
Subscribe to the quarterly safety and data quality briefing. Validation readouts, design partner cohort updates, and conference timing only. No tracking beacons, no marketing email cadence.